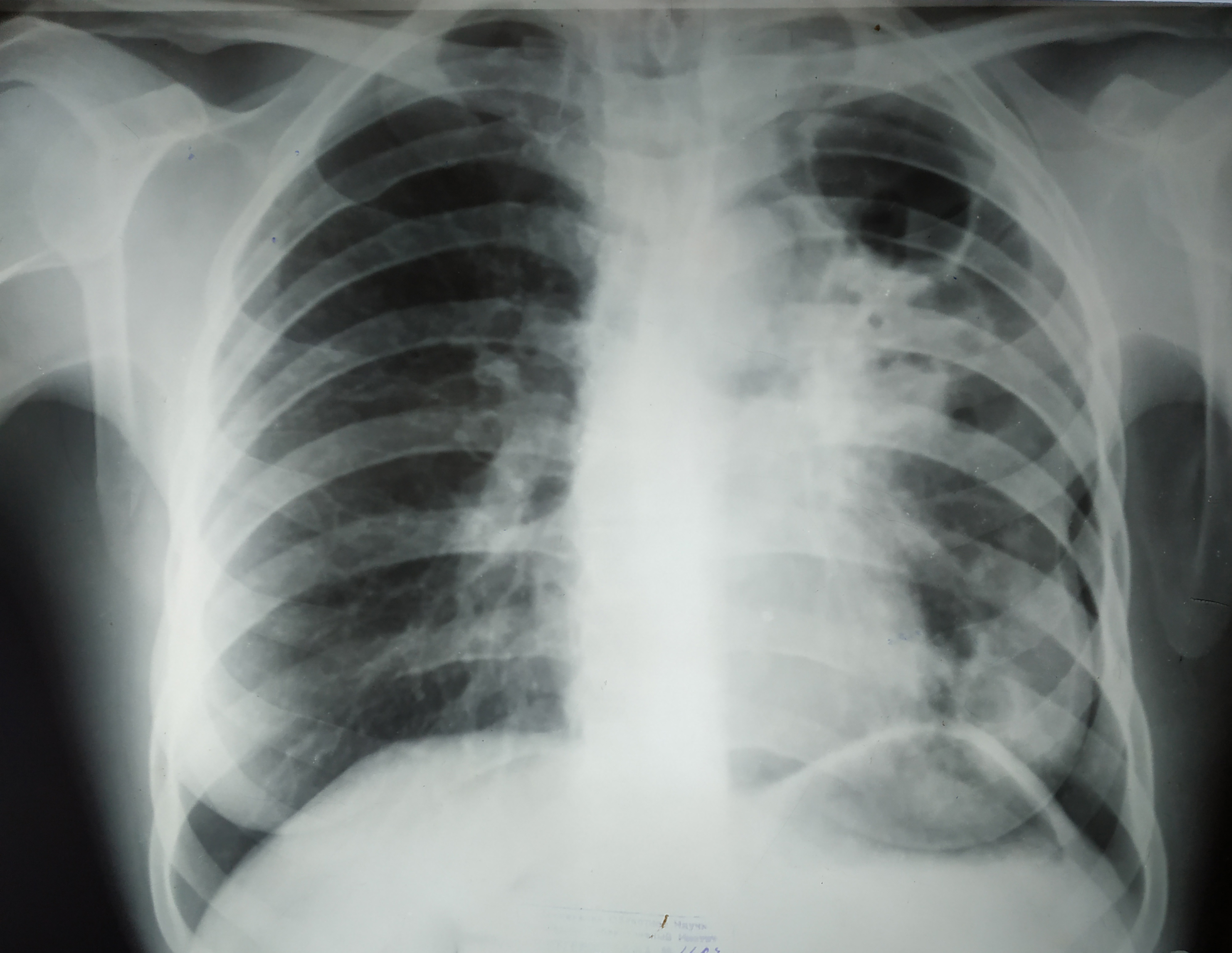
Pulmonary Tuberculosis
From sequelae to drug-resistant disease - the thoracic surgeon's role in the management of PTB.
Overview
Surgery was historically the primary treatment for pulmonary tuberculosis (PTB) - collapse therapy, thoracoplasty, and plombage were widely used before the antibiotic era. With the discovery of streptomycin in 1943 and subsequent introduction of combination chemotherapy, surgery retreated to a secondary role. In the current era, surgery is indicated for sequelae of PTB, complications, and drug-resistant disease.
Pulmonary tuberculosis is caused by Mycobacterium tuberculosis - a rod-shaped, aerobic, acid-fast bacillus characterised by slow multiplication and the capacity for dormancy over decades. The lung is the most commonly affected organ, accounting for approximately 80% of all TB.
Pathogenesis
Primary pulmonary TB
Following airborne infection, a subpleural granuloma forms in the distal airways - the Ghon focus. When accompanied by tubercular lymphangitis and hilar lymphadenopathy, this constitutes the Ghon complex. On healing, the calcified subpleural lesion with calcified hilar lymph node forms the Ranke complex. In immunocompromised patients, primary TB may progress to consolidation, lymphadenopathy, pleural effusion, or miliary disease.
Post-primary (reactivation) TB
Reactivation usually occurs within two years of primary infection, typically affecting upper lobe parenchyma. It leads to cavitation and consolidation. Healing produces fibrosis, scarring, volume loss, traction bronchiectasis, and potential pleural involvement.
Surgical indications
| Category | Specific indications |
|---|---|
| Sequelae of PTB | |
| Lung parenchyma | Destroyed lung · Persistent cavity · Aspergilloma |
| Airway | Tracheobronchial stenosis · Broncholithiasis · Bronchiectasis |
| Complications | |
| Haemoptysis · Lung abscess · Pneumothorax · Empyema · Bronchopleural fistula | |
| Drug-resistant TB | |
| MDR-TB | Resistance to isoniazid and rifampicin ± other first-line drugs |
| XDR-TB (2021 WHO) | MDR/RR-TB + resistance to any fluoroquinolone + at least one of bedaquiline or linezolid |
| Atypical mycobacterial infection (NTM) | |
| Localised resectable disease · Persistent positive cultures · Destroyed lung | |
A multidisciplinary approach - infectious disease specialists, respiratory physicians, radiologists, and thoracic surgeons - is essential for timing and patient selection, particularly in drug-resistant disease.
Surgical management of PTB sequelae
Destroyed lung
Complete parenchymal destruction in end-stage TB, more commonly affecting the left lung. Pathogenesis involves chronic inflammation, cicatrisation atelectasis, fibrosis, cavitation, and repeated secondary infection. Indications for pneumonectomy include recurrent infections, haemoptysis, failure to thrive, and recurrent TB.
Pneumonectomy in TB-destroyed lung is technically demanding: thickened or calcified pleura, hilar fibrosis, loss of normal tissue planes, and enlarged lymph nodes encasing vessels. Extra-pleural dissection and intrapericardial vascular control are frequently required. Bronchial stump reinforcement is mandatory in all cases - options include intercostal muscle flap, pericardial fat pad, omentum, or pedicled muscle flap (latissimus dorsi, pectoralis major, diaphragm). Post-pneumonectomy empyema and bronchopleural fistula are the most common major complications.
Persistent cavity
Most tubercular cavities resolve with chemotherapy. Persistent cavities may be thin-walled (mimicking bullae) or thick-walled. Chronic cavities risk relapsing TB, aspergilloma formation, and Rasmussen aneurysm. Indications for surgery: haemoptysis, aspergilloma, and persistence despite adequate chemotherapy. Anatomical resection (lobectomy) is preferred over wedge excision.
A false aneurysm caused by progressive weakening of bronchial or pulmonary artery walls adjacent to a TB cavity. Granulation tissue replaces the adventitia and media, then is replaced by fibrin, causing pseudoaneurysm formation and eventual rupture - a major cause of life-threatening haemoptysis in cavitary TB. Treatment is anatomical lobar resection; bronchial artery embolisation may serve as a bridge.
Tracheobronchial stenosis
Left main bronchus is most commonly involved. Pathogenesis: healed endobronchial TB causes submucosal granuloma, ulceration, and stricture. Management depends on the extent of airway involvement and condition of the lung parenchyma. Isolated stenosis with preserved lung may be managed with bronchoscopic dilatation (recurrence is common). Parenchyma-sparing bronchoplastic procedures are preferred for limited disease; lobectomy or pneumonectomy for destroyed or significantly diseased lung.
Broncholithiasis
Calcified tubercular lymph nodes eroding into the bronchial lumen, causing obstruction. Mobile broncholiths may be removed bronchoscopically. Fixed broncholiths require bronchotomy, removal, and repair.
Drug-resistant PTB - surgical role
The 2021 WHO updated definition of XDR-TB defines it as MDR/RR-TB with additional resistance to any fluoroquinolone plus at least one of bedaquiline or linezolid. The previous definition (resistance to any fluoroquinolone + one of the second-line injectables) is now superseded.
Surgical resection as an adjunct to chemotherapy may provide better outcomes in selected cases - particularly where drug therapy alone is unlikely to achieve sputum negativity or where there is localised resectable disease. Pre-operative optimisation to achieve sputum negativity or reduced bacillary load is strongly desirable before elective resection.
Drug regimens for MDR-TB and XDR-TB evolve rapidly with new agents (bedaquiline, delamanid, pretomanid). For current WHO-recommended treatment regimens, refer to the WHO Consolidated Guidelines on Tuberculosis (2022).
Non-tuberculous mycobacteria (NTM)
NTM (also known as MOTT - mycobacteria other than tuberculosis) are ubiquitous environmental organisms. Both immunosuppressed and immunocompetent hosts may be affected. MAC (M. avium complex), M. kansasii, and M. abscessus are the most common respiratory pathogens.
Surgical indications in NTM: relapse or re-infection with localised resectable disease; persistent positive cultures despite adequate chemotherapy; or destroyed lung parenchyma (bronchiectasis, fibrocavitary disease).
Drug selection and duration for NTM infections depend on species, susceptibility, and clinical context. For current protocols, refer to the ATS/ERS/ESCMID/IDSA Clinical Practice Guidelines for NTM (2020).
All clinical content should be verified against current guidelines before clinical application. This resource is intended for revision and educational purposes only.
Standard textbooks
- Shields TW, LoCicero J, Reed CE, Feins RH. General Thoracic Surgery. 7th ed. Lippincott Williams & Wilkins.
- Sellke FW, del Nido PJ, Swanson SJ. Sabiston & Spencer Surgery of the Chest. 9th ed. Elsevier.
- Pearson FG, et al. Thoracic Surgery. 3rd ed. Churchill Livingstone.