Lung Abscess
Liquefactive necrosis of lung parenchyma - when conservative management fails and surgery is required.
Necrosis of pulmonary tissue with cavity formation (>2 cm) containing debris and fluid, due to microbial contamination. Acute: <6 weeks duration. Chronic: >6 weeks duration.
Pathophysiology and aetiology
Necrotising pneumonia leads to liquefactive necrosis of lung parenchyma. Central necrosis liquefies and communicates with the bronchial tree, producing the classic air-fluid level cavity on imaging.
| Setting | Common organisms |
|---|---|
| Aspiration (most common) | Bacteroides, Peptostreptococci, Fusobacterium - anaerobes predominate |
| Immunocompromised | Klebsiella, Enterobacter, Pseudomonas, Proteus, Staph aureus |
| HAP/VAP/Elderly/HIV | Gram-negatives, Aspergillus, Actinomycosis, Nocardia, Amoeba |
Common locations: Aspiration abscesses preferentially affect the posterior segment of the RUL, superior segment of the RLL, and left lower lobe - the dependent segments in the recumbent position.
Investigations
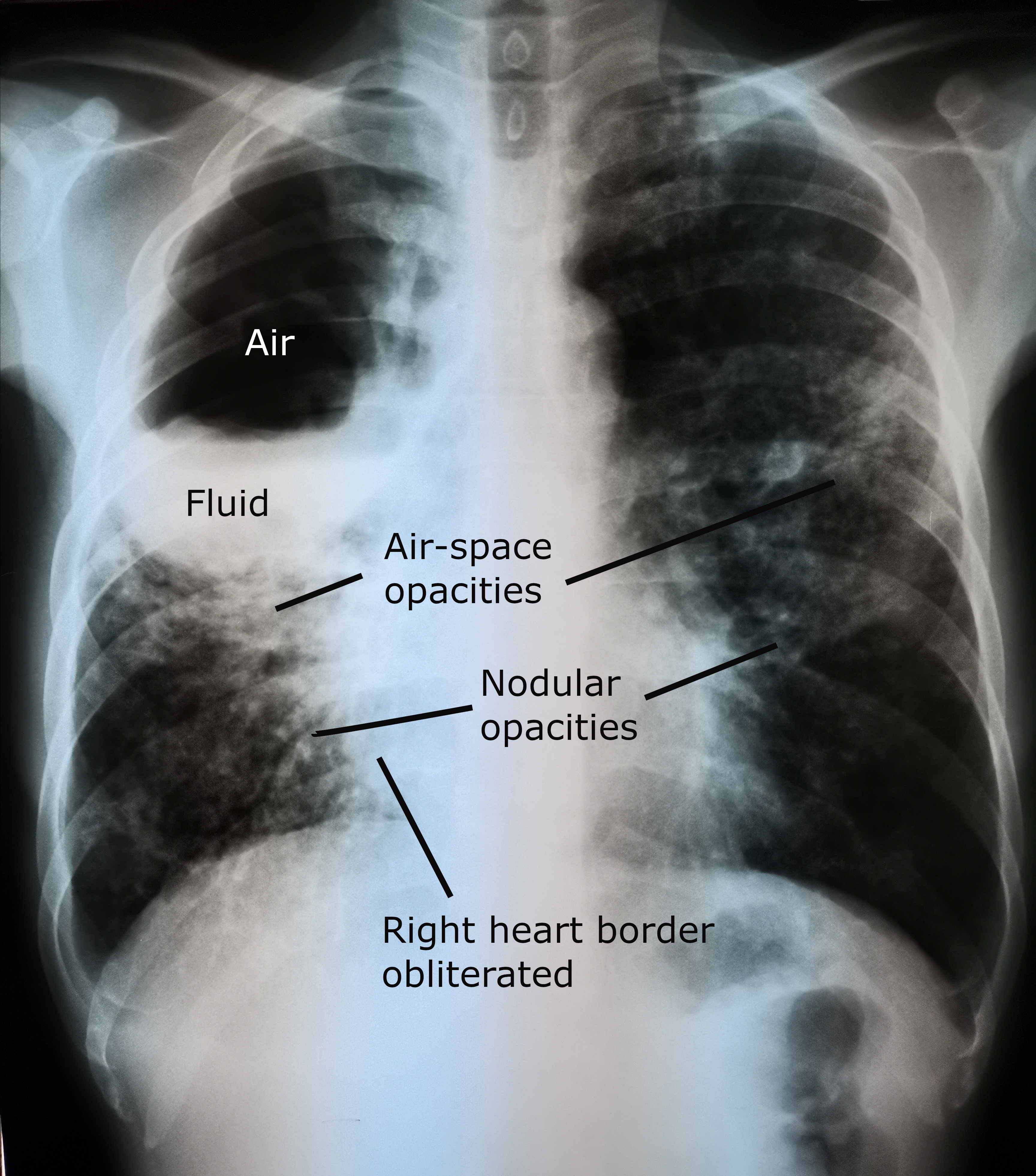
- Chest X-ray: consolidation early; classic rounded cavity with air-fluid level when communication with bronchial tree established
- CT thorax: characterises the abscess, identifies associated pathology, guides drainage
- Bronchoscopy: rules out bronchial obstruction (tumour, foreign body) and facilitates drainage
- Sputum/pus analysis: aerobic, anaerobic, fungal, and TB cultures
Treatment
Medical management
Antibiotic selection depends on causative organism, resistance patterns, and clinical context. Refer to local or national guidelines (e.g., NICE or BTS) for current recommended regimens. Duration is typically 4–6 weeks minimum.
Percutaneous drainage
Performed under radiological guidance (ultrasound, fluoroscopy, or CT). Indicated when:
- No improvement after 1–2 weeks of antibiotics
- Solitary, enlarging abscess >6 cm
- Imminent rupture risk
- Contamination of contralateral lung threatened
- Microbiological diagnosis needed
Surgery
Standard indications (lung resection - lobectomy/pneumonectomy):
- No improvement with treatment >6 weeks (chronic lung abscess)
- Size >6 cm
- Sepsis persisting >2 weeks
Special indications:
- Haemoptysis
- Suspicion of underlying malignancy
- Associated bronchopleural fistula
- Associated empyema requiring surgical management
Lung abscess surgery carries higher risk than elective resection - contaminated field, suppurated lung, and risk of soiling the contralateral lung. Careful lung isolation with a double-lumen tube or bronchial blocker is essential before entering the chest. Anatomical resection (lobectomy) is preferred over wedge or non-anatomical excision.
All clinical content should be verified against current guidelines before clinical application. This resource is intended for revision and educational purposes only.
Standard textbooks
- Shields TW, LoCicero J, Reed CE, Feins RH. General Thoracic Surgery. 7th ed. Lippincott Williams & Wilkins.
- Sellke FW, del Nido PJ, Swanson SJ. Sabiston & Spencer Surgery of the Chest. 9th ed. Elsevier.
- Pearson FG, et al. Thoracic Surgery. 3rd ed. Churchill Livingstone.